Youth Crisis Response System Training RFA Q&A
The Center for Evidence to Practice held a Live Question & Answer session in October 2023 on the new Louisiana Youth Crisis Response System (LA-CRS) Training and the Request for Applications (RFA) that was released in September 2023. Below is a recording of the webinar and a summary of the questions asked and answers given. If you have additional questions
You can view the PowerPoint Slides here.
Question: What will provider enrollment with Managed Care Entities (MCEs) look like? Will an agency have to amend their current contracts if they are already credentialed with the MCEs to provide outpatient behavioral health services?
Answer: Agencies have to be credentialed and contracted with all Medicaid MCOs and the CSoC Contractor to provide Youth Crisis Response Services. For questions about your contract, we recommend contacting the MCE directly. The provider will need to contract as a mobile crisis response and a community brief crisis support provider, in addition to obtaining a Crisis Receiving Center – Level III (Freestanding) or a Behavioral Health Services Provider license from the LDH Health Standards Section (HSS) identifying the provider as a mobile crisis provider.
Question: What are the lessons learned from the implementation of adult crisis response services that might assist in the implementation of the youth crisis response system services?
Answer: 1. Readiness is key. Providers expressing interest that showed lower readiness scores on their applications have consistently struggled or failed to implement. The Center would rather help such agencies become ready as opposed to joining the training when they are not ready. 2. Provider agency understanding that this is a new state endeavor requiring a system shift. The Center makes every attempt to ensure that agency administrations and clinical supervisors understand what they are taking on in regards to a substantial culture shift in Louisiana’s crisis response system. Unlike in the initial launch of the adult system, we will have agency leadership training in the youth implementation phase, prior to training agency’s frontline staff. 3. Community relationships are crucial to implementation and success. Providers must be committed to developing and maintaining local partnerships within the communities they are serving. There will be an emphasis on developing relationships in the community. This is a collective and collaborative effort to launch these services. Having relationships with law enforcement, local governing entities (LGEs), and schools will be essential. Every system in Louisiana looks different depending on the community needs and their local culture.
Question: How have transfers from the MCE crisis lines or 988 gone within the adult system?
Answer: As the development of the adult system progressed, it was clear that most agencies benefited from accepting direct referrals, when possible, versus going through the MCE crisis lines. The MCE crisis lines remained active and serve a purpose, but both local calling and the addition of the 988 call lines and transfers increased utilization. The state continues to work toward a statewide crisis hub, to work in conjunction with 988, providers, MCEs and local partners, which is a model many states are taking. Other options that have been attempted with varying degrees of success have been including behavioral health crisis response in the options for local 911.
Question: The Louisiana Youth Crisis Response System aims to provide crisis response services to youth who are Medicaid-insured. What about the youth that are not Medicaid-insured?
Answer: Agencies with diversified funding (i.e., funding sources in addition to Medicaid) seem to implement services, with greater volume, faster. Medicaid is important as a major funder of these regional efforts, but the overall business models of agencies benefit from braided funding. Additionally, in the adult rollout of services, the state created grant opportunities for agencies to temporarily serve individuals without Medicaid. This approach may be repeated for the youth system, but that will depend on the availability of funding and the impact observed from the pilot in the adult system.
Question: What would an agency do if you have a youth in crisis and are unable to get their provider on the phone or their provider doesn’t offer crisis intervention?
Answer: It depends. If the person has a provider, the preference will always be to attempt to have that person connect with their existing provider for continuity of care, including providing crisis mitigation services required by licensure. Providers should always take the first line of response to the people they are offering care to. However, the Louisiana Crisis Response System will serve a youth in crisis when the existing provider is not available or responsive. They will continue to connect that person with their established provider as safely and efficiently as possible, though.
Question: Are any current providers seeing reimbursement issues?
Answer: In the implementation of the adult model, the providers, MCEs, the Center, and LDH-OBH have been in consistent contact to discuss any implementation issues multiple times monthly, including billing issues. This process will continue with the youth system providers. The successful implementation of these services is a priority for the state, so having an expedited opportunity to jointly review what is working and what are challenges is imperative.
Question: Will agencies need a behavioral health license in place prior to the application or will prior to services in Spring 2024 be acceptable?
Answer: No. A CRC-Level III or BHSP license is not required prior to submitting an application, however agencies must be licensed prior to implementing services in Spring 2024. However, it should be noted that agencies with a history of successful licensing with the state are certainly more aware and ready for those necessary steps.
Question: Are certain areas in more need than others?
Answer: We don’t have that answer yet. With the adult training RFA for example, Region 5 has proven to be a challenge to find providers that are ready to provide adult crisis response services. We believe much is due to the extensive provider shortage in that area following several major disasters. Rural areas of the state have also seen lower interest (as indicated by fewer applications for training) compared to more suburban/urban areas.
Question: Are you looking for programs to respond to mental health crises in school systems?
Answer: The new youth mobile crisis response (MCR) teams will be expected to respond to youth crises in homes and schools, in addition to other places where youth are in the community (e.g., foster care homes, group homes). MCR teams will be expected to build relationships with local schools and school districts to support effective response options. Agencies will be encouraged to formalize relationships with schools, and other institutions, with locally developed MOUs (memorandums of understanding).
Question: Does an agency have to a get new license if you have an MCR/CBCS BHSP or CRC-Level III license already?
Answer: No, a new license will not be required.
Question: May a provider be contracted to cover several regions, or will each region require a separate contract?
Answer: Providers may contract for more than one region. Providers will need to communicate directly with the MCEs to determine the steps required to either amend existing contracts or initiate new contracts. However, agencies with the ability to demonstrate capacity to serve multiple regions are also likely to be more ready to enter training. Although this isn’t a guarantee of readiness, providers may select as many regions as they are hoping to serve on the application.
Question: Are rural areas given any special considerations? Do you anticipate the need to be less or greater in different areas of the state?
Answer: When considering applying, keep in mind that these are regional services. We need providers, who are prepared to provide services to the entire area of a region, including the rural areas. To accommodate additional travel time needed in rural areas, there are different required response times for crisis teams responding to urban vs. rural areas.
Question: Staffing requirements state a Medical Doctor must be on 24hr call; however, when looking in the program/clinical components, there is no mention of use of a Medical Director (MD). How are MDs used in this model?
Answer: Mobile crisis response and community brief crisis support services require a medical director or a designated prescriber, i.e., APRN or medical psychologist, to be available for consultation and medication management to address individualized needs of clients that may go beyond the scope of non-medical staff.
Question: Is there a way to expedite the BHSP license process to assist with preparing to provide this service if selected as a provider?
Answer: HSS has an expedited licensing process. The following link is provided as a resource for further information on the expedited licensing process: http://ldh.la.gov/index.cfm/newsroom/detail/5010
Question: Will start-up funding be available?
Answer: A limited amount of funding may be available for qualified providers that have successfully completed training, are licensed by HSS as a BHSP mobile crisis response provider or CRC Level III and credentialed and contracted with all MCEs. Providers must be implementing services before consideration is given for any available temporary start-up funding. Start-up funding is not guaranteed.
Question: Is the training outlined on the training RFA information page? (i.e., time requirements, licensed professionals needed, etc.)?
Answer: Yes, the training is outlined in the training RFA. We do attach CEHs to this training, so if staff are licensed they will be able to take advantage of these CEHs as an additional benefit for their time.
Question: Do the youth crisis services require prior authorization?
Answer: MCR services are a response to an immediate crisis and therefore do not require prior authorization. The CBCS, which are the 15-day follow-up services, currently require prior authorization.
Question: Is LDH-OBH promoting programs for response to crises in school systems?
Answer: Yes. We understand from states that have implemented youth crisis services for many years, the two primary callers for youth crisis services are schools and families. The Center is emphasizing this in its training focus and LDH-OBH is prioritizing the school environment in its collaboration and policy development efforts.
Question: Have there been barriers with MCEs approving or prior authorizing services?
Answer: In the implementation of the adult model, the providers, MCEs, the Center, and LDH-OBH have been in consistent contact (i.e., multiple times monthly) to discuss any implementation issues, including billing issues. This includes discussing approving and/or authorizing service issues. This process will continue with the youth system providers. The successful implementation of these services is a priority for the state, so having an expedited opportunity to jointly review what is working and what are challenges is imperative.
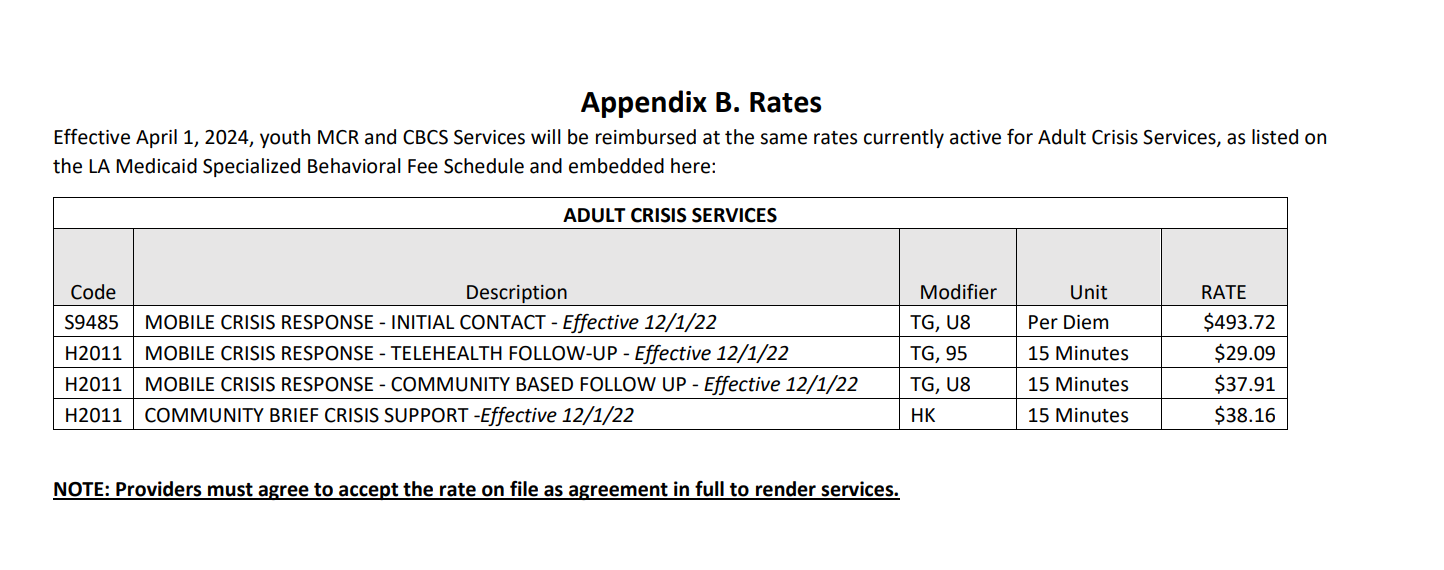
Question: Is the rate sheet with effective dates 12/1/22 correct?
Answer: Current approved rates for services can be found here.
{kind=link}